
AI-Powered Thinking for Dental Practice Owners
A practical guide to building your AI think team — the methodology, the lens for choosing what to build, and the ten specialists every practice should have.
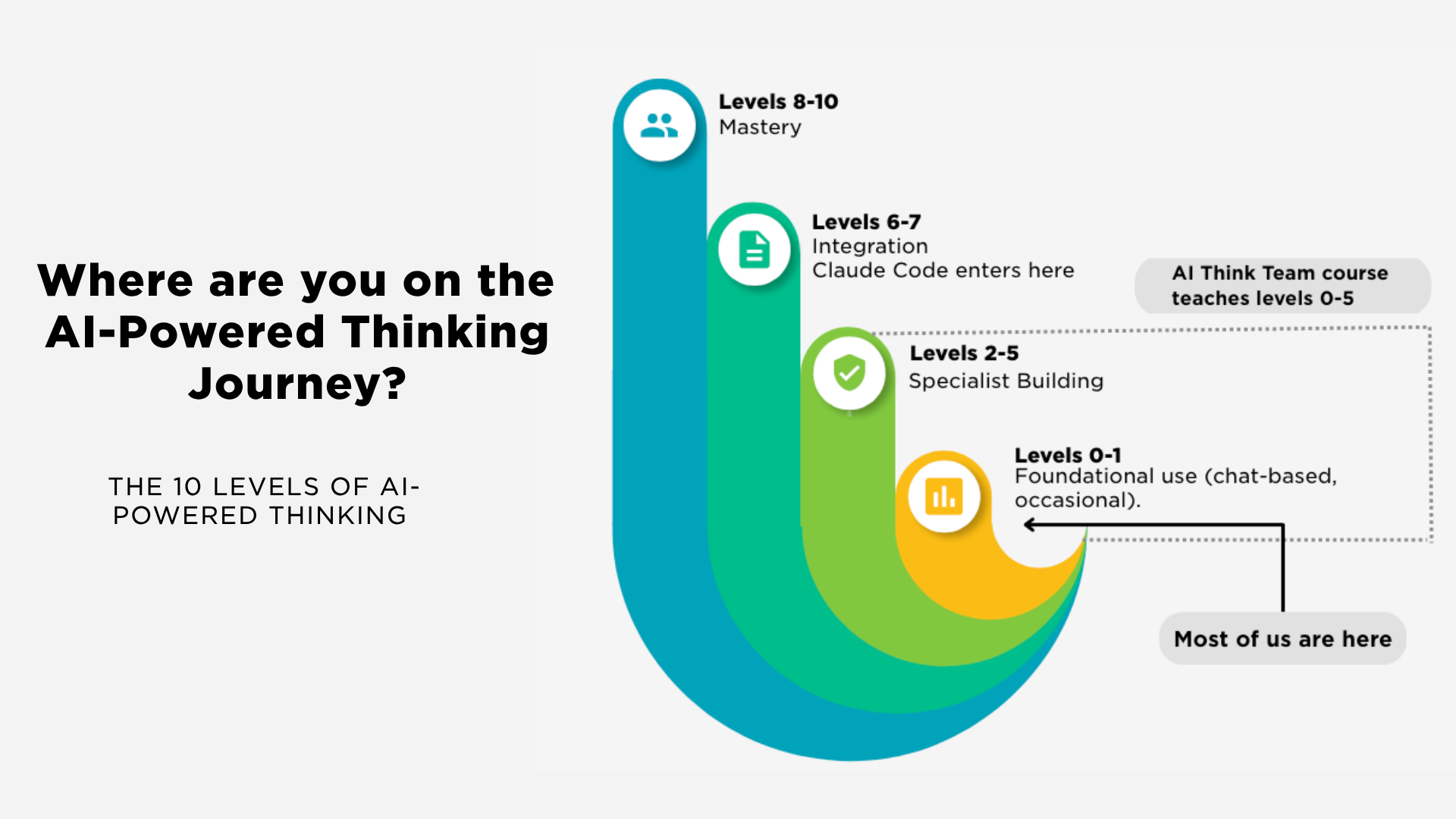
Table of Contents▼
Most dentists who try AI bounce off because they're using it to do tasks. The ones pulling ahead are using it to think. Here's the practical methodology, the framework, and the ten specialists every practice should have.
Why most dentists stall with AI
You have probably already tried this. Most dentists have. You opened ChatGPT, or Claude, or Gemini, asked it to draft a recall message or tidy up a patient letter or summarise a policy, and what came back was usable. Not bad. Not the thing that reshapes your week either. Somewhere around the third or fourth attempt, a quiet verdict settles in: AI is fine, occasionally handy, and a long way short of what everyone keeps promising.
That verdict is far more common than the noise around AI would suggest. I once asked a room of 82 dentists a simple pair of questions. 72% had used AI in the past month. Around 10% had built it into a working part of the practice. Almost everyone had walked through the door. Very few had done anything with the room once they were inside.
That gap is the whole story, and it is worth being precise about what it is not. It is not an access gap; the tools cost around $20 a month and most dentists already have a login. It is not a willingness gap; 72% is a high number. The gap is what happens after the first few prompts. Most people try AI, get an adequate result, decide adequate is the ceiling, and stop.
The dentists in that 10% were not working with better software. Same ChatGPT, same subscription, same models available to everyone else in the room. What set them apart was what they had decided AI was for. Most dentists use it to do tasks. The ones pulling ahead use it to think. The distinction sounds slight. It is the entire difference between the experience you have probably already had and the one this guide is about.
Most dentists use AI to do tasks. The ones pulling ahead use it to think.
Why automation alone fails
Some dentists do not stop at mild disappointment. They decide the problem is that they have not gone far enough, and they reach for automation: a tool that runs the whole task without them, a system that does the job end to end. The instinct is reasonable. It also tends to disappoint, and the reason is worth understanding before any money changes hands.
In my experience the underlying problem is three patterns running together: broken processes underneath, vague prompts on top, and front-end tools bolted on without back-end integration. Automation accelerates whatever you give it. If the process behind the tool is unclear or inconsistent, automation produces the same unclear, inconsistent output, only faster and in greater volume. You can't automate noise.
The chatbot interface most people start with is part of the bottleneck. Ethan Mollick, the Wharton professor whose work on practical AI use is among the most widely read, calls this capability overhang: the distance between what these systems can already do and what most people think to ask of them. A scratchpad for quick tasks is not the same as a built system that runs a workflow reliably, and the difference becomes obvious the moment you try to run any real part of a practice on it.
I run 65 AI specialists daily, and I have not turned any of them into autonomous agents. That is deliberate. The order matters: build, then trust, then automate. Skipping straight to automation is the move that produces the underwhelming result most dentists have already met.
AI-powered thinking is the ceiling
The reframe is in two words: thinking, not tasks. The dentists I have watched build something genuinely useful with AI did not start by asking it to do their work for them. They started by using it to think alongside them.
I will be straightforward about how I use it myself. I treat AI as a way to borrow somewhere between 50 and 80 IQ points on demand. That is not modesty. It is a description of what good use of these systems looks like, even for someone already operating at the top of their field.
Mo Gawdat, the former Google X executive who has spent the last decade on AI's social effects, frames it more sharply than I would. AI, he says, is either going to make you dumb or the smartest you have ever been. There is no neutral position. Whether the system makes you sharper or duller depends almost entirely on how you use it.
The trap in the middle is the echo chamber. These systems are trained on human feedback, and most of that feedback rewards agreeableness. Ask a chatbot whether your idea is good, and it will, on average, tell you it is good. Ask it to find the flaws, and it might list a few generic ones. The default behaviour reinforces whatever you already think.
I deal with this by running a specialist whose entire job is to disagree with me. Its default is to take the opposite position to whatever I bring it. When I am convinced of a strategic move, its first job is to make the strongest case against it. The point is not to be contrarian. It is to surface the blind spots before the move gets made.
The thinking ceiling is higher than the task ceiling. A specialist that drafts your treatment plan letters saves time. A specialist that genuinely challenges your strategy, your hiring decisions, or the way you have been thinking about case acceptance changes the quality of what you decide.
The lens: finding your specialists
Once you accept that AI is more useful for thinking than for tasks, the next question is which thinking jobs to give it. The filter I use, which I call the Lens, is three questions long.
Does the task repeat? Can you describe what good output looks like? Could you teach a thoughtful outsider to do it?
Three yes answers means it is a job worth giving an AI specialist. Anything less, and the task either does not need a specialist or needs a person.
The same three questions apply to your next hire. If a job repeats, has describable output, and could be taught, you have a choice between hiring a human and building a specialist. The Lens does not say which is right; it says the question is real either way.
Treatment plan follow-up is a clean example. The task repeats every time a patient leaves with a multi-stage plan. Good output is a clear summary of the plan, the rationale, the financial figures, and the next step the patient should take. A thoughtful outsider could be taught to produce it, given the case notes and the practice's tone of voice. Three yeses. That is a specialist.
I have watched a clinician build exactly this. The specialist generates a tailored summary for each patient, with QR codes that link to short educational videos relevant to that patient's specific concerns. The clinician reviews and sends. The patient leaves the chair with something that explains, in their own language, what was discussed and what comes next. The Lens is what stopped her building a specialist for the wrong job first.
A three-question filter for deciding which thinking jobs to give an AI specialist. Does the task repeat? Can you describe what good output looks like? Could you teach a thoughtful outsider to do it? Three yes answers means it is a job worth giving a specialist.
The two-layer methodology
Knowing what to build is half the work. The other half is building it well, and the methodology I use has two layers. The first layer is for individual conversations; the second is for permanent specialists that you and your team use again and again.
The 4 C's solve any individual prompt. Most weak prompts are missing two of the four. Most strong ones include all four in two or three sentences.
The 4 C's
| The 4 C's | What it covers |
|---|---|
| Context | What the model needs to know about your situation |
| Content | The source material it should work from |
| Command | The specific instruction you want it to follow |
| Constraints | The rules and boundaries that keep the output usable |
For permanent specialists, you go a layer deeper. The BRIEF is a five-part structure that turns a one-off prompt into a colleague the system can play whenever you call it.
The BRIEF
| Letter | Element | What it does |
|---|---|---|
| B | Build identity | Tells the specialist who it is |
| R | Role context | Tells it the world it operates in |
| I | Instructions | What it does |
| E | Evaluation criteria | How it knows whether the output is good |
| F | Few-shot examples | Shows it what good looks like in practice |
I think about the difference as briefing an intern. The instructions are the brief you give an intern on day one. The knowledge files are the manual you tell them to consult when they get stuck. A well-built specialist has both, and the difference between a mediocre specialist and a strong one usually sits in the few-shot examples and the knowledge files, not in the instructions themselves.
The BRIEF travels across platforms. Claude has Projects. ChatGPT has Projects. Gemini has Gems. Each one is a different name for the same thing: a container that holds the BRIEF and the knowledge files and lets the specialist run consistently across multiple conversations.
One flag worth raising before you build anything patient-facing. Patient data needs to be anonymised before it goes into a general-purpose AI system. The Business Associate Agreements that put HIPAA-compliant tooling in place are usually enterprise-tier features. Treat patient-facing specialists with appropriate caution; a BRIEF for treatment plan letters is fine when the case data has been stripped of identifiers, less fine when it has not.
Patient data must be anonymised before it goes into a general-purpose AI system. The Business Associate Agreements that make tooling HIPAA-compliant are usually enterprise-tier features. Treat any patient-facing specialist with caution — strip identifiers from case data first.
Start with the Identity Builder. It is the foundation specialist, the one every other specialist references. Build that one well, and the rest of the team gets easier to build.
Your AI think team: the ten specialists
Put the methodology into operation and you end up with a working AI think team of about ten specialists. Ten is not a magic number. It is roughly the count where most of a practice owner's repeating decisions and outputs are covered. Here are the ten roles I would build, in the order I would build them.
| # | Specialist | What it does |
|---|---|---|
| 1 | The Identity Builder | The foundation. Encodes your practice's positioning, voice, and core principles in a form every other specialist can reference. |
| 2 | The Brand Voice Engine | Extends the identity into how the practice communicates externally — across emails, social, and patient-facing copy. |
| 3 | The Treatment Presentation Builder | Produces patient-facing summaries of treatment plans, financial breakdowns, and educational content. The one with the HIPAA caveat. |
| 4 | The Insurance Appeals Writer | Drafts the response letters for denied claims, drawing on the case notes and the reasoning behind the original recommendation. |
| 5 | The Content Machine | A chain of specialists rather than a single one. Several run in sequence: one develops the raw idea, the next shapes the structure, the next produces the finished asset. |
| 6 | The Financial Analyst | Sits across practice numbers and answers the questions the dashboard does not — production trends, profitability per chair, the pattern behind a slow month. |
| 7 | The Decision Partner | The strategic-thinking specialist. Captures the reasoning behind a major decision and surfaces the blind spots before the decision is final. |
| 8 | The SOP Builder | Turns a working process into a written standard operating procedure the team can follow without the original architect in the room. |
| 9 | The Team Coach | Supports your one-to-one meetings — records the conversation, prepares for the next one, summarises what was covered, suggests coaching moves. |
| 10 | The Hiring Manager | Sits across the practice's hiring needs, drafts job descriptions in the practice's voice, and helps screen candidates against the role. |
I run 65 specialists daily across my own work. Ten is the starter set, not the limit. Four of them earn their place every single week. One captures the reasoning behind a decision and tells me what I have missed before I commit to it. One prepares and debriefs my team one-to-ones so the coaching is consistent. One is the content chain that produces most of what I publish. And one exists only to disagree with me, so that nothing important goes ahead without its weakest point being named first. You do not need 65. You need the right ten, and then the few that turn out to matter most to you.
Where to start
Three moves to take this week.
First, take the three questions from the Lens and run them across the work that fills a typical week in your practice. Does the task repeat? Can you describe what good output looks like? Could you teach a thoughtful outsider to do it? The tasks that earn three clear yeses are your specialist candidates. The honest part is doing this against the real list of what occupies your week, not in the abstract.
Second, read the Dental Practice AI Starter Guide. It takes the candidates you have just identified and maps them to the specialist worth building first, with the starting structure and build order so the work is concrete rather than open-ended.
Third, build one specialist. Iterate it for two weeks before adding a second. My recommendation for a first build is either the Identity Builder, because every other specialist will reference it, or the SOP Builder, because the act of building it forces you to write down the working processes that have only ever lived in someone's head.
You do not have to build all ten. The build, trust, automate sequence applies to the team itself. Get one specialist working well, trust what it produces, then add the next.
If you are ready to build the full team and want the structured walkthrough, I teach the methodology end to end in Your AI Think Team. Ten modules, around seven hours, seven CE credits, on-demand and self-paced. $495 to enrol with a $20 monthly fee for ongoing access. The course covers each of the ten specialists in detail with the BRIEF, the knowledge files, and the use cases for each one.
The shift is operational
The shift is not technical. It is operational.
The dentists who are pulling ahead are not the ones with better tools. They are the ones who have rebuilt the way their practices think. The tools came later. The thinking came first, and the methodology that put it on a footing they could actually run from sat underneath all of it.
The distance between the experience most dentists have had with AI and the one this guide describes is not measured in budget or in software. It is one well-built specialist, then the next. The first takes a few hours. The second is faster. By the third, the pattern is yours, and what you are running is less a handful of one-off prompts and more a team that thinks alongside you.
Frequently Asked Questions About AI for Dental Practices
What does "AI-powered thinking" mean for a dental practice?
AI-powered thinking means using AI as a thinking partner — to pressure-test decisions and surface blind spots — rather than as a tool that only completes isolated tasks. It is the difference between a time-saver and a genuine change in the quality of what a practice owner decides.
Why do most dentists stall with AI?
Most dentists stall not because of cost or unwillingness — the tools are cheap and adoption is high — but because they stop after the first few prompts, having decided an adequate result is the ceiling. The gap is structure: the dentists getting leverage from AI use it to think, not just to do tasks.
Why doesn't automation alone fix the problem?
Automation accelerates whatever process it is given, so automating an unclear or inconsistent process simply produces unclear, inconsistent output faster. The reliable order is build, then trust, then automate.
How do I decide which tasks to give an AI specialist?
Use the Lens — a three-question filter: does the task repeat, can you describe what good output looks like, and could you teach a thoughtful outsider to do it? Three yes answers means the task is worth giving to an AI specialist.
How many AI specialists does a dental practice need?
A practical starter team is about ten specialists — roughly the count that covers most of a practice owner's repeating decisions and outputs. You do not build all ten at once; you build one, trust it, then add the next.
Is it safe to put patient data into AI tools like ChatGPT?
Patient data should be anonymised before it goes into any general-purpose AI system. HIPAA-compliant tooling requires a Business Associate Agreement, usually available only on enterprise-tier plans, so patient-facing specialists need extra caution.
Where should a practice owner start with AI?
Run the Lens across the work that fills a typical week to identify your specialist candidates, then build a single specialist — usually the Identity Builder or the SOP Builder — and iterate it for two weeks before adding another.
Continue Learning

Ready to build your AI think team?
Start with one specialist this week. The Dental Practice AI Starter Guide gives you the build order, the BRIEF templates, and the use cases for all ten — free.
Get the Starter Guide