
How to Build a Dental Practice That Grows Without You
The most capable person in your practice is also your biggest operational risk. Here is the system that removes the dependency: two engines, six systems, and the guide that helps you build them in the right order.


Table of Contents ▼
A case acceptance system is the set of repeatable, non-clinical processes — spanning lead generation and database activation — that turn prospective and existing patients into booked treatment without depending on any single person. In most practices the most capable person is also the biggest operational risk, because the entire system lives in their head. The output looks excellent, which is exactly why the risk stays invisible until the day that person is busy, sick, or gone.
This guide lays out the architecture that removes that dependency: two engines, six systems, and a clear order to build them in. The aim is a practice that keeps following up, converting, and asking for the review whether or not your best person came in today.
The one-sentence test that finds your weakest system
Here is a test you can run on your practice today. Pick any process that isn't clinical. Following up on a treatment plan. Calling back a lead. Asking a happy patient for a review. Now ask one question: does this happen because we have a system, or because a particular person remembers to do it?
If the honest answer is that someone remembers, you don't have a system. You have a person holding everything together.
That person is usually your best person. Often it's the owner. Sometimes it's an office manager who has been there for years and simply absorbs the work nobody else thinks about. The output looks excellent, which is exactly why the risk is invisible. The better the hero, the more dangerous the dependency, because nobody can see the gap until the day that person is busy, or sick, or gone. When they're busy, the follow-up waits. When they're sick, it stops. When they leave, it walks out the door with them, and they take the whole system with them because the system was only ever in their head.
I want to be clear about what I'm saying, because it's easy to hear this as a criticism of the people doing the work. It isn't. A hero is not a failure of effort. A hero is a design gap. The question that exposes it isn't "who handles this?" The right question is "do we have a system for this?" The first question keeps you dependent. The second one starts to set you free.
A hero is not a failure of effort. A hero is a design gap.Brendon MacDonald, CEO, DSD
Two engines, six systems, one flywheel
When you map out everything that has to happen between a stranger noticing your practice and that stranger becoming a patient who refers their friends, it sorts cleanly into two engines.
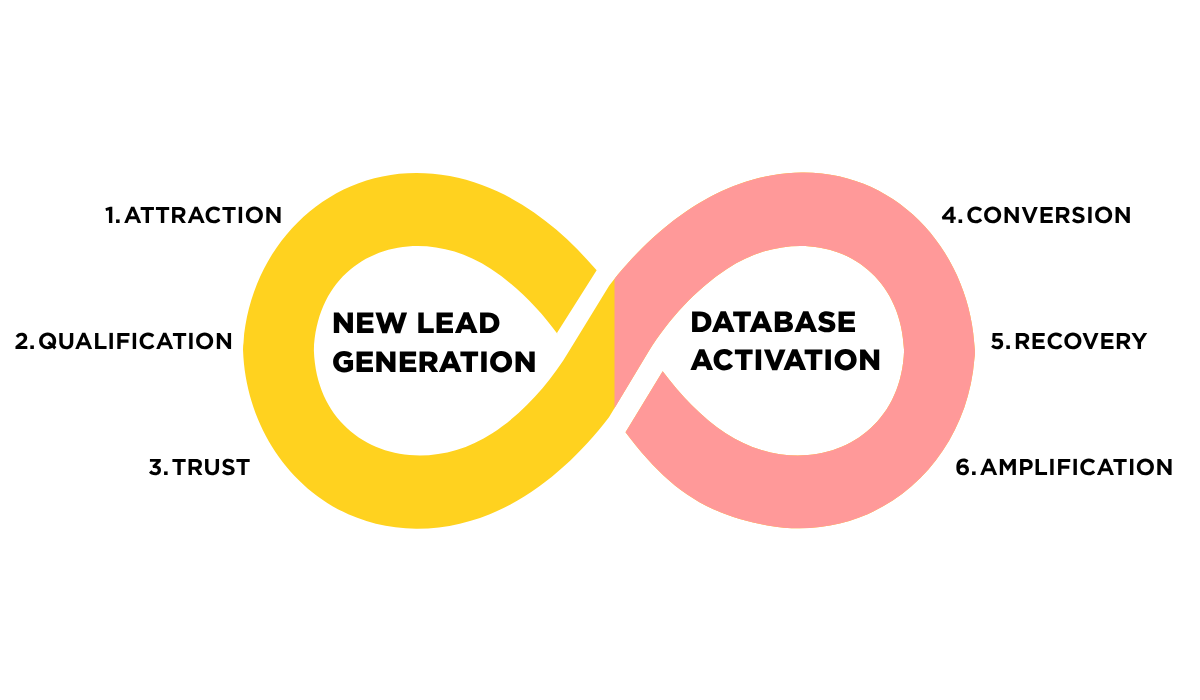
Engine one is new lead generation. It has three systems: attraction, qualification, and trust. This is the work of finding people who don't know you yet and earning enough of their confidence to get them through the door.
Engine two is database activation. It also has three systems: conversion, recovery, and amplification. This is the work of turning the people you already have in front of you into booked treatment, and turning the ones who said no into the ones who eventually say yes.
Six systems, two engines. The reason I draw it as a flywheel rather than a funnel is the last system. Amplification, the reviews and referrals you generate from happy patients, feeds directly back into attraction. A funnel ends. A flywheel turns. When the sixth system is working, it makes the first system cheaper and easier, and the whole thing starts to compound. That's the architecture. The rest of this page is about why most practices have one or two of these systems running well and four of them barely running at all.
A funnel ends. A flywheel turns.Brendon MacDonald, CEO, DSD
| Engine | System | The job it does |
|---|---|---|
| New lead generation | Attraction | Finding people who don't know you yet |
| New lead generation | Qualification | Responding fast and triaging hot / medium / cold |
| New lead generation | Trust | Filling the booking-to-consult gap so they show up |
| Database activation | Conversion | Recovering the 60% who say "I'll think about it" |
| Database activation | Recovery | Reactivating lapsed patients before 18 months passes |
| Database activation | Amplification | Turning happy patients into reviews and referrals |
Why attraction is almost never the problem
If I ask a room of practice owners to name their single biggest pain, around 90% say the same thing: we need more leads. More new patients. More at the top of the funnel.
I understand the instinct, and I spent years on the other side of it. Before this, I owned a dental marketing agency. So I know exactly what the lead-generation conversation sounds like, and I know what actually happens after the leads arrive. Here is what I learned: attraction is not your problem.
Finding leads is relatively easy now. The tools are good, the targeting is good, and you can turn the tap on this afternoon if you want to. What you do after the lead arrives is the hard part, and that is where almost every practice is losing money. The real problem is systems two to six.
This matters because pouring more leads into a practice with no follow-up capacity doesn't fix anything. It multiplies the frustration. The agency believes it delivered, because it did. The practice sees no new patients, because the leads fell through the gaps between people. Both sides blame each other, and the cycle repeats. I watched it happen from the agency side more times than I'd like to admit. If your follow-up systems aren't live, more leads just means more leads going to waste.
There's a financial trap inside this too. Paid media is like a drug. Once you're on it, it's very hard to come off, because it's a once-off hit every time: you stop paying, the patients stop coming. Practices that put 80% of their budget into paid media without the follow-up systems to convert it watch their return collapse, then spend more to chase it. The fix isn't more spend. The fix is to build systems two to six first, so that every lead you already pay for actually turns into something. There's a quiet piece of good news underneath all of this. Small practices were always told what the ideal follow-up plan looked like, but they never had the capacity or the budget to run it. Technology has closed that gap. The capacity barrier that kept good follow-up out of reach is gone, which means a small practice can now run the same systems a large group runs.
Speed wins, and silence is expensive
Picture your patient filling out an enquiry form at 9:15 on a Tuesday night. Three practices receive it. Practice A does nothing until someone gets in the next morning. Practice B fires off an autoresponder. Practice C responds within 60 seconds with a real conversation, not a robot, a genuine reply that answers the question the patient actually asked.
Who wins? Around 78% of patients go with whoever responds first. And the average response time for an enquiry in North America is 47 hours. So of course Practice C wins. It isn't close. The standard worth holding yourself to is a 60-second first response, qualified, 24 hours a day. In practice that means an AI-first response within 60 seconds, human-enhanced for roughly 80% of cases, with your team picking up the hot leads first thing in the morning when they come in to leads that are already worked and full of context.
The cost of not doing this is not abstract. For a practice doing around $3 million, the silence between an enquiry and a response is worth about $265,000 a year. That's $265,000 lost not because of bad clinical work, but because of silence. Nobody did anything wrong clinically. The phone just didn't get answered fast enough.
The silent gap before the consult
Speed gets them to book. The next system, trust, gets them to actually turn up. There's a gap between the moment a patient books and the day of the consult, and that gap is silent in most practices. The longer the silence, the higher the no-show rate. A same-day appointment carries roughly a 2% no-show rate. By 15 days out it's around 33%, climbing about 4% for every extra day of waiting. A no-show is not a lost consultation fee. It's the lost treatment, the lost lifetime value of that patient, and up to 12 months of revenue that never arrives.
The answer to the silent gap is what I call communication zero: a planned sequence of messages that fills the wait with trust instead of doubt. Eight emails over about 12 days, fewer if the appointment is sooner, each doing one specific job. Introduce the doctor. Tell the story and the values. Show social proof. Answer the common questions. Handle insurance. Cover the logistics. Explain what to expect. The single most anxiety-reducing thing you can tell a patient before a big consultation is that no treatment will happen at this visit. And here's the part most practices miss: if you ask permission at booking, those eight emails feel expected and welcome, not like spam. The patient chose 12 days of trust over 12 days of silence.
Communication zero: A planned sequence of around eight emails over roughly 12 days that fills the wait between booking and consult with trust instead of doubt — each message doing one job, from introducing the doctor to handling insurance.
Ask permission for the communication-zero sequence at the moment of booking. When the patient opts in, the emails feel expected and welcome rather than like spam — they chose 12 days of trust over 12 days of silence.
"I'll think about it" is not a no
Around 60% of consultations end with some version of "I'll think about it." Most practices hear that as a soft no and quietly write the patient off. That is one of the most expensive habits in dentistry.
"I'll think about it" is not a no. And it's not even one objection. It's actually six. When you record and transcribe consultations and look at what's really going on, the deferrals break down into six barriers. Roughly 45% are financial. Around 25% are about needing to discuss it with a spouse or partner. Then there's fear, the desire for a second opinion or to shop around, a sense that it isn't urgent or isn't a priority right now, and finally the genuine no. Only the last group is actually finished. Around 40% of consults say yes on the day; the other 60% defer, and most of that 60% is recoverable.
| Barrier | Share of deferrals | The right response |
|---|---|---|
| Financial | ~45% | Payment options, financing, value framing |
| Spouse / partner | ~25% | Materials they can share and discuss at home |
| Fear | Part of remainder | No urgency — empathy, nervous-patient testimonials |
| Second opinion / shopping | Part of remainder | Reinforce credibility and differentiation |
| Not urgent / not a priority | Part of remainder | Keep the door open via the recovery system |
| Genuine no | Part of remainder | The only group that is actually finished |
For a practice doing $2 to $3 million and running 400 to 500 consultations a year, that deferred backlog adds up to around $1.5 million in treatment plans sitting there, annually. Not lost. Sitting there. A systematic follow-up recovers something like 30 to 40% of it.
The reason most practices don't recover it is that they rely on a hero to remember to follow up, and the hero is busy. Meanwhile the patient forgets the doctor's name by about day seven. The fix is a contextual 30-day follow-up that triggers automatically, runs in three phases, and starts by finding out which of the six barriers you're actually dealing with. Your team classifies the barrier and makes two calls; the system runs the rest from a library of message templates matched to the barrier type.
The "contextual" part is not a nice-to-have. It's the whole thing. If a patient's barrier is fear and you respond with urgency, you make it worse. The fear branch needs the opposite: no urgency, more empathy, testimonials from nervous patients who came through it, reassurance. Apply a financial-objection sequence to a fearful patient and you'll lose them faster than if you'd said nothing. So you don't guess. You ask, or you go back to the transcript, and you run the sequence that fits.
Two messages do most of the closing work. The first one, sent soon after they leave, while the consultation is still fresh. And the final one, the breakup message, the one that says you're closing their file and you won't keep chasing them. Around 50% of the people who get a well-written breakup message actually go ahead. It works because it releases a small amount of low-grade guilt and, paradoxically, gives the patient permission to act.
The breakup message: The final follow-up in the conversion sequence — it tells the patient you're closing their file and will stop chasing. Around 50% of recipients of a well-written one go ahead, because it releases low-grade guilt and gives them permission to act.
The cheapest patient you'll ever win
When a 30-day follow-up doesn't convert, most practices go quiet. That silence is the mistake, because if you lose contact with somebody for 18 months, you've genuinely lost them. Before that, they're still yours to win back, and winning them back is the best economics in your practice.
The cost to reactivate someone who already knows you is about $5 to $15. The cost to acquire a fresh lead is $150 to $300. The cheapest patient you'll ever win is the one you already have. That's what the recovery system is for, and the most important thing to understand about it is what its job is not. Recovery is not about closing. The moment you treat a reactivation campaign as a closing push, you apply pressure to someone for whom the treatment simply wasn't a priority, and pressure pushes a non-priority patient further away. Recovery's job is to keep the door open, so that when life changes, and it does, they come back to you rather than starting over with someone else.
In practice that's a four-wave cadence across 12 months. A 30-day rest after the conversion sequence ends, then a seven-day sequence at day 60, again at day 120, and so on, with incentives that rise the longer the relationship has been quiet. Layer in seasonal reasons to reach out: the insurance benefit reset, tax-refund season, a birthday, the new year. When someone responds, they aren't "closed". They re-enter the qualification system as a live lead, and your team picks up the alert with the full history in front of them. A simple email newsletter is one of the most effective recovery tools there is, for the plain reason that everyone receiving it already raised their hand once. Most patients who deferred never end up doing the treatment with anyone. It wasn't that they chose a competitor. It just never became a priority. Recovery is how you stay the practice they think of on the day it finally does.
The cheapest patient you'll ever win is the one you already have.Brendon MacDonald, CEO, DSD
Your patients want to refer you. You're just not asking
Here are two numbers that should bother you. Around 83% of happy patients intend to refer you. About 29% actually do. And 68% intend to leave a review, while only 7% do.
Sit with the size of that gap. The motivation is already there. More than eight in ten of your happy patients want to send you their friends. The gap isn't the motivation. It's the infrastructure. The practice simply never built the ask into a system, so the intention quietly evaporates between the chair and the car park.
Amplification is the system that closes that gap, and it has to be built carefully, because the rules here are not optional. There are two compliant approaches. Approach A is proactive: you send an NPS survey to everyone, then a review link to everyone. You cannot gate it. Done well it generates around 8 to 10 reviews a month and builds a moat of social proof that's very hard for a competitor to catch. The one caution is that it's risky when you have fewer than 50 reviews, because the volume isn't there yet to absorb a stumble. Approach B is reactive: you use the NPS survey for insight, then ask for a public review only from the patients who volunteer that they had a great experience.
| Approach A — Proactive | Approach B — Reactive | |
|---|---|---|
| Method | NPS to everyone, then review link to everyone | NPS for insight; ask only volunteers who report a great experience |
| Output | ~8–10 reviews / month | Lower volume, higher safety |
| Best when | You already have a review base | Under 50 reviews |
| Never do | Gate reviews (review link only to high scorers) — non-compliant, often illegal | Same |
What you must never do is gate reviews, meaning run an NPS survey and then send the public review link only to your high scorers. That is non-compliant and, in many places, illegal. The compliant version of using the score is about tone, not gatekeeping: when a score comes back low, you soften and redirect privately to fix the problem; when it comes back high, you encourage the public review. Your team moves a card; the system handles the outreach.
One more reason volume matters. When you have fewer than 50 reviews, a single bad one can drag a 4.9 down to a 4.2. Once you've built a real base of reviews, that same bad review becomes a non-event. Volume is its own protection.
And this is the system that closes the flywheel. The reviews and referrals you generate here feed straight back into attraction, making the very first system cheaper and more effective. That's why it's a flywheel and not a funnel. The sixth system powers the first.
Never gate reviews — running an NPS survey and then sending the public review link only to your high scorers. It is non-compliant and, in many jurisdictions, illegal. Use the score for tone, not gatekeeping: soften and redirect low scores privately; encourage public reviews from high scores.
Who owns it
A system that depends on no single hero still depends on clearly owned seats. The difference is that the work lives in defined roles and a running cadence, not in one person's memory, so any individual can be replaced without the system leaving with them.
There are four core seats, plus an optional fifth. A system owner, which is usually the office manager and is the natural home for the cadence and the seasonal calendar. A lead responder, who owns qualification: the 60-second response, the triage into hot, medium, and cold, working the hot leads first. A case coordinator, the treatment or case coordinator, who owns conversion and responds to recovery alerts. A clinical voice, for the moments that genuinely need clinical credibility. And optionally a marketing coordinator.
There is one split you must never collapse. The lead responder and the case coordinator are two different jobs, and the temptation in a smaller practice is to hand both to one person. Resist it. Qualifying a brand-new enquiry at speed and shepherding a deferred high-value case through a 30-day sequence are different skills with different rhythms, and folding them into one seat is how both get done at half strength.
The reason this works without a hero is the hybrid model. For every one of the six systems, you draw a clear line between what the system handles automatically and what the team does by hand. The automatic side runs the cadence, sends the sequences, fires the alerts, and never forgets, because it isn't remembering, it's running. The human side does the things that genuinely need a person: the two calls, the judgement on a tricky barrier, the clinical reassurance. Get that line right for each system and you have a practice that keeps following up, keeps converting, and keeps asking for the review whether or not your best person came in today.
So go back to the one-sentence test you started with. Run it across all six systems. Wherever the honest answer is "because someone remembers," you've found a system to build. The guide shows you how, and points you to a scored diagnostic, four questions per system, so you know exactly which one to fix first.
Frequently Asked Questions About Case Acceptance Systems
What is a dental case acceptance system?
A case acceptance system is the set of repeatable, non-clinical processes — across lead generation and database activation — that convert prospective and existing patients into booked treatment without relying on one person remembering to act. It's built from six systems across two engines: attraction, qualification, trust, conversion, recovery, and amplification.
How fast should a dental practice respond to a new patient enquiry?
The standard worth holding is a qualified first response within 60 seconds, 24 hours a day. Around 78% of patients book with whoever responds first, yet the average enquiry response time in North America is 47 hours — making speed one of the cheapest competitive advantages available.
Why do dental patients say "I'll think about it"?
"I'll think about it" is rarely a single objection — it breaks down into six barriers: financial (~45%), needing to discuss with a spouse (~25%), fear, wanting a second opinion, low urgency, and the genuine no. Only the last group is truly finished; a contextual follow-up recovers 30–40% of the rest.
How much does it cost to reactivate a lapsed dental patient?
Reactivating a patient who already knows you costs about $5–15, compared with $150–300 to acquire a fresh lead. The cheapest patient you'll ever win is one you already have — provided you reach them before roughly 18 months of silence passes.
How do you reduce no-shows for dental consultations?
No-shows climb with the silent gap between booking and the appointment — from about 2% same-day to 33% at 15 days out. The fix is "communication zero": a planned sequence of around eight emails over 12 days, agreed at booking, each doing one job from introducing the doctor to handling insurance.
Is it legal to ask only happy patients for online reviews?
Gating reviews — running an NPS survey and sending the public review link only to high scorers — is non-compliant and illegal in many jurisdictions. Compliant practices either ask everyone (proactive) or ask only patients who volunteer a great experience (reactive), using a low score to redirect privately rather than to filter who gets asked.
How many people does it take to run a case acceptance system?
A case acceptance system runs on four core seats plus an optional fifth: a system owner, a lead responder, a case coordinator, a clinical voice, and optionally a marketing coordinator. The one rule you can't break is keeping the lead responder and case coordinator as separate jobs — qualifying fast and shepherding deferred cases are different skills.
Continue Learning


Build your six systems in priority order
Find the weakest one first, then build them in order. The six-system guide shows you how and points you to a scored diagnostic.
Download the six-system guide Not ready to download? Keep exploring the learning hub for more on building a practice that grows without you.